

5 Signs Your Hip Pain May Be Gluteal Tendinopathy, Not Arthritis
If three or more of these signs sound familiar, the diagnosis you were given could be inaccurate.

If you have pain on the outside of your hip that started during or after menopause, and you have already tried the usual treatments without long-term relief, there is a strong possibility you were never given the correct explanation.
Not every point below will perfectly match your situation. But if at least three of them do, what you are experiencing is very likely different from what you have been told. And that difference may explain why nothing has worked for long.

1. The pain is on the OUTSIDE of your hip, not deep in the groin
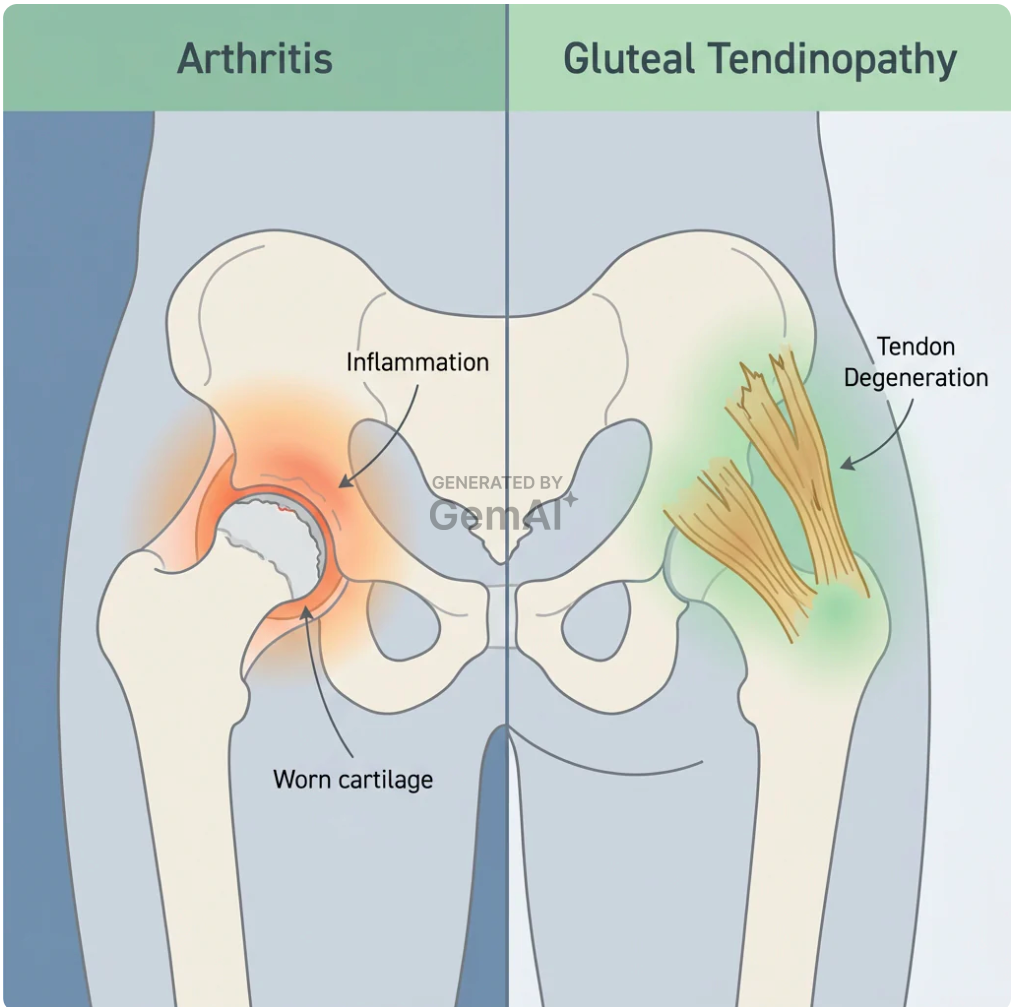
Arthritis develops inside the hip joint itself. It usually causes pain in the groin area, sometimes spreading down the inner thigh. In most cases, it progresses slowly over many years as cartilage gradually wears away.
Gluteal tendinopathy affects the outer part of the hip instead. It is the side you sleep on. The area that throbs after sitting too long, hurts when you roll over at night, or stiffens when you stand up after being seated for half an hour.
If your pain is mainly on the outside of the hip, but you have been told it is arthritis, those findings do not fully line up. And if your X-rays appear normal, arthritis becomes even less likely, because joint arthritis is usually visible on imaging. Tendon damage often is not.

2. Your imaging came back normal, or showed only “mild age-related changes”
Arthritis is usually visible on X-rays. It often appears as joint space narrowing, bone spurs, or changes in the cartilage surface. If arthritis is significant, a radiologist will typically identify it.
Gluteal tendinopathy, however, often does not appear on standard X-rays. So when a doctor reviews your scan, says there is “nothing significant,” but still labels it arthritis, those conclusions do not fully fit together.
A normal scan does not necessarily mean nothing is wrong. In many cases, it is actually an important clue pointing somewhere more specific. It may suggest the problem is in the tendons rather than the joint itself. Tendons are soft tissue, which means they usually cannot be seen clearly on regular X-rays. To properly evaluate tendon health, an ultrasound or MRI with soft tissue detail is often needed, yet many women with this kind of hip pain never receive either.

3. The pain gets worse the longer you stay in one position, not better
Arthritis typically causes morning stiffness that improves once you start moving. If you have arthritis and walk around for ten or fifteen minutes, the joint often loosens up and feels less stiff over time. Movement usually helps.
Gluteal tendinopathy often behaves in the opposite way. The longer you remain in one position, the more stress builds on the tendons, and the more painful the area becomes. Sitting at a desk for too long can make the hip ache sharply when you stand up. Lying on that side at night may cause the pain to deepen the longer you stay there.
If your doctor advised you to walk more and your symptoms became worse instead of better, this may explain why. Exercise is commonly recommended for arthritis because movement supports joint function. But when tendons are already degenerating and struggling to repair themselves, repeatedly loading them without addressing the underlying tissue problem can increase irritation rather than relieve it.

4. The pain appeared suddenly during or shortly after menopause
Arthritis usually develops slowly over many years of joint wear and tear. It does not commonly appear suddenly in your late 40s or early 50s without a long history of symptoms beforehand.
Gluteal tendinopathy can develop much more rapidly because the trigger is often hormonal rather than purely mechanical. Estrogen plays a major role in collagen production, which is the structural protein that helps tendons stay strong and repair themselves after everyday strain. When estrogen levels decline during menopause, the tendons around the hips can lose much of that repair support very quickly.
If your hip pain began within a year or two of noticeable hormonal changes, and you sensed there was a connection even if your doctor dismissed it, that pattern may not be accidental. It closely matches what the biology suggests can happen during menopause. Estrogen declines, collagen production slows, tendon resilience weakens, and pain can gradually follow.

5. Cortisone, anti-inflammatories, and physical therapy helped briefly, then stopped working
Cortisone injections and NSAIDs are designed to reduce inflammation. For a short period, they may decrease swelling and calm the pain response. But after a few weeks, the relief often fades and the pain returns to the same area. This cycle can continue because those treatments may not address what is happening inside the tendon tissue itself. Inflammation is often a response to tendon degeneration, not always the root cause. Treating only the inflammation without supporting tissue repair can be like drying the floor while the leak above is still active.
Physical therapy strengthens the muscles around the hip, and for many conditions that approach is extremely helpful. But when tendon degeneration is linked to estrogen-related collagen decline, strengthening exercises alone may not fully address the deeper tissue changes taking place. You can improve the surrounding muscles, yet the tendon underneath may still struggle if its structural quality has weakened.
That does not mean the treatments were universally wrong. It means they may not have been the right fit for this specific issue.
If most of these signs match your experience, there is a strong chance you are not dealing with arthritis at all. What you may actually have is gluteal tendinopathy — a gradual breakdown of the hip tendons that can be influenced by the hormonal changes of menopause and the decline in estrogen.
Arthritis and gluteal tendinopathy require very different treatment approaches.
Many of the treatments that failed to provide lasting relief may have been designed for a different condition altogether. That does not mean those options were wrong in general — they may simply have been aimed at the wrong target.
Gluteal tendinopathy is linked to changes in tendon health and collagen repair. Because of that, approaches focused only on reducing inflammation, strengthening nearby muscles, or improving comfort may not fully address the underlying tissue changes involved.
Women who eventually experience long-term improvement are often the ones who shift their focus from only managing symptoms to supporting tendon recovery itself. Addressing the tendons directly means understanding what the tissue actually needs in order to repair and function more effectively. Today, there are emerging non-surgical approaches designed to support tendon health without injections or additional medications, and some can be done in short daily sessions at home.
“I stopped asking why nothing had worked and started asking what the tendons actually needed. Those are different questions with different answers.”


Many of the women who recognized their own symptoms in these five signs had previously been told they were dealing with arthritis, bursitis, or simply “normal” imaging results. The diagnosis was not incorrect because their pain was imaginary. It was incorrect because the underlying condition causing the pain had never been properly identified.
Recognizing the real source of the problem is the first step. Understanding how to address it comes next.
The Information Your Doctor May Never Have Connected

Treating gluteal tendinopathy at the source means supporting repair directly within the tendon tissue itself — not only through oral medications, and not through short-term injections that may wear off after a few weeks, but by targeting the area where the breakdown is occurring.
That is the idea behind Kalsten Device. It is a wearable hip wrap that includes an integrated therapeutic light panel designed for short daily use. The system uses three targeted wavelengths, each intended to support a different aspect of tendon recovery:
Kalsten was created specifically for women in perimenopause and post-menopause experiencing persistent outer hip pain that has not improved with standard approaches. It is positioned as a targeted support device rather than a general wellness product.The page below explains the connection many women with this type of pain are never told about, and what makes Kalsten HerStride different from conventional treatment options.